How is chronic cough treated?
Management of chronic cough
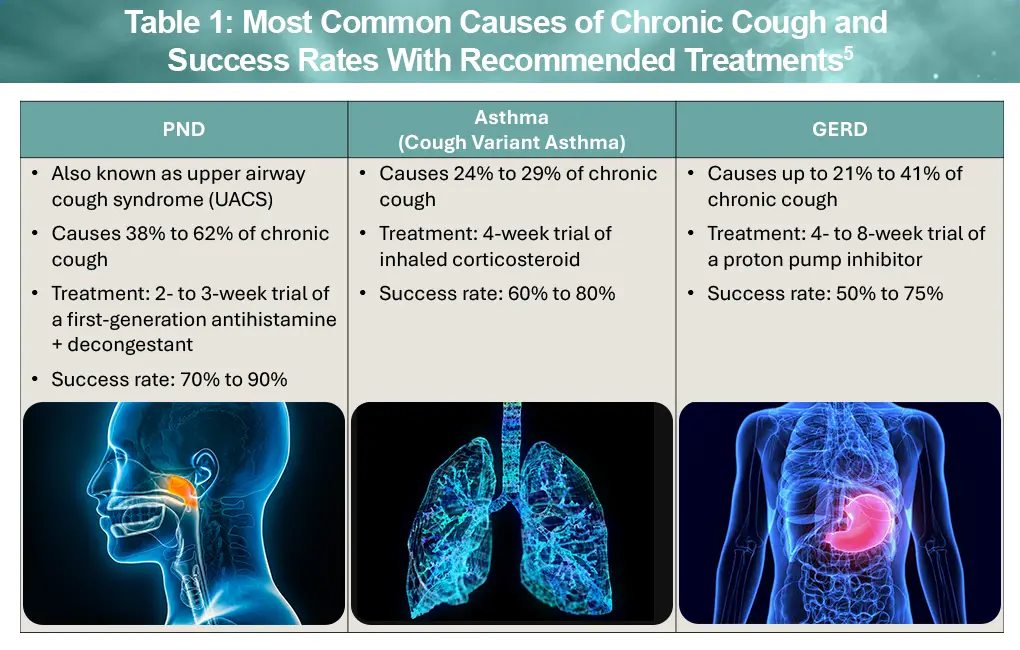
Management of chronic cough involves a stepwise approach that begins with identifying and treating the underlying cause. After ruling out red flags for serious medical conditions and medications as the cause, your healthcare provider (HCP) will focus on the three most common causes of chronic cough—asthma, postnasal drip (PND), and gastroesophageal reflux disease (GERD)—which account for 90% of chronic cough in nonsmokers. In most patients, evaluation for each of these will be done one at a time, followed by a trial of recommended medication. Table 1 shows the percentage of patients affected by PND, asthma, and GERD, and the success rates with recommended therapies.1-4
In some people, cough does not improve despite treatment of these common causes. Approximately 10% to 30% of people don’t experience relief from their chronic cough after recommended treatments for PND, asthma, and/or GERD. Typically, these patients are referred for evaluation by a specialist.5
Possible causes of chronic cough in these patients include5:
- Chronic bronchitis: seen in tobacco smokers
- Pertussis: also known as whooping cough, uncommon in adults
- Chronic aspiration: breathing in food, liquid, or saliva
- Eosinophilic bronchitis: airway inflammation without typical asthma features
- Refractory chronic cough (RCC): caused by cough hypersensitivity
RCC may be related to more than one cause, including overlapping cough hypersensitivity, even early on in the disease. The term “postnasal drip” is now more often referred to as upper airway cough syndrome, or UACS, as it reflects not just mucus but the increased sensitivity of the cough reflex. In a similar way, “silent reflux” is increasingly recognized as different from classic GERD. Laryngopharyngeal reflux (LPR) does not cause heartburn but occurs when acid reaches the throat and voice box. Patients with LPR also experience chronic cough.5
Although stress does not directly cause RCC, it can make it worse. If your cough reflex is already hypersensitive, as can happen with asthma, GERD, or LPR, stress may increase that sensitivity. Treating the underlying cause remains important, but stress management strategies may help reduce flare-ups.5
Recommended therapies for RCC
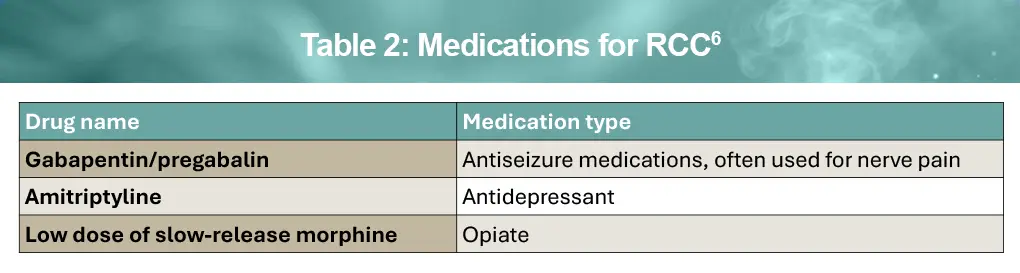
Right now, there is no FDA-approved therapy for RCC. However, your HCP may talk with you about the potential benefits and side effects of certain medications that have been found to reduce the symptoms of chronic cough in small clinical trials. You can expect to try the medication for a couple of months to see if there is any change in your cough. Table 2 highlights medications that can be used to treat RCC.6
Emerging therapies for RCC
After decades of limited treatment options for RCC, new therapies that target the nerve pathways involved in cough hypersensitivity are on the horizon. Drugs belonging to a class called P2X3 antagonists have shown promise for RCC and are designed to block stimulation of airway receptors that contribute to excessive coughing. Gefapixant is the first P2X3 antagonist to be approved but it is not available in the United States.7,8 Another P2X3 antagonist, camlipixant, is currently in late-stage clinical trials and has been reported to be effective with few side effects.9-11
Nalbuphine, an oral κ-opioid receptor agonist/μ-antagonist, has also demonstrated promising activity and moved into late-stage clinical evaluation. Other new drugs being studied include sodium channel blockers, TRPM8 inhibitors, neurokinin 1 antagonists, and GABAB agonists, reflecting high interest in developing new therapies for RCC.9,10
Behavior modification therapy for RCC6,12
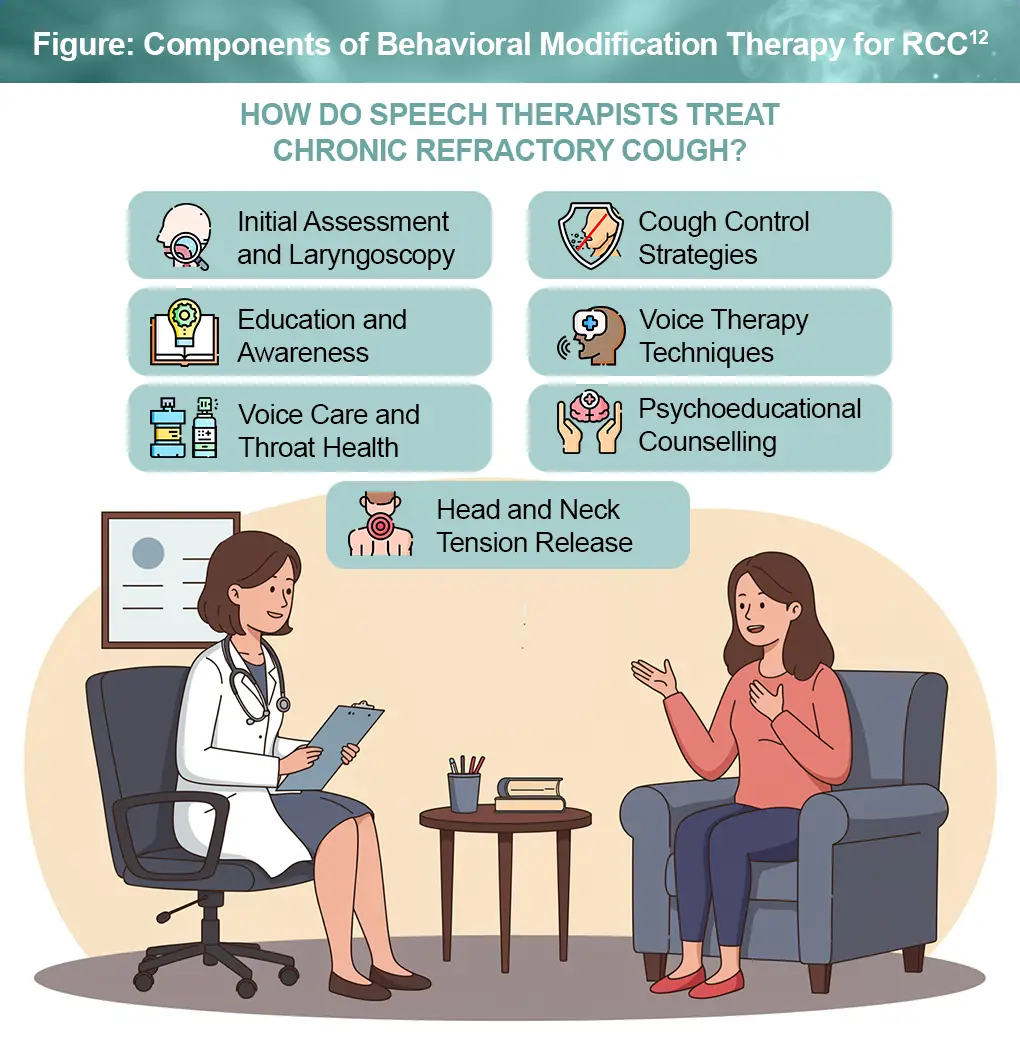
Behavior modification involves teaching patients with RCC techniques to control their cough. This type of therapy is typically delivered by a speech and language specialist, and includes education, strategies to suppress the cough reflex, training on vocal hygiene, and counselling.
Behavior modification teaches the patient strategies to suppress their cough, using swallowing or relaxed breathing techniques. Such specialists also help to identify what causes the cough, how to avoid triggers, and how to manage anxiety related to persistent coughing. The Figure shows how speech therapists work with patients with RCC to deliver behavioral modification therapy.
References
- Satia I, Hassan W, McGarvey L, et al. The clinical approach to chronic cough. J Allergy Clin Immunol Pract. 2025;13:454-466.
- Gibson P, Wang G, McGarvey L, et al. Treatment of unexplained chronic cough: CHEST Guideline and Expert Panel Report. CHEST. 2016;149:27-44.
- Irwin RS, French CL, Chang AB, et al. Classification of cough as a symptom in adults and management algorithms: CHEST Guideline and Expert Panel Report. CHEST. 2018;153:196-209.
- Morice AH, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur Respir J. 2020;55:1901136.
- Chronic cough workup: how to diagnose GERD, asthma, and postnasal drip. December 15, 2025. https://spbappo.com/chronic-cough-workup-how-to-diagnose-gerd-asthma-and-postnasal-drip
- Canadian Lung Association. Breathe. Chronic cough. https://www.lung.ca/lung-health/lung-diseases/chronic-cough
- McGarvey LP, Birring SS, Morice AH, Dicpinigaitis PV, et al. Efficacy and safety of gefapixant, a P2X3receptor antagonist, in refractory chronic cough and unexplained chronic cough (COUGH-1 and COUGH-2): results from two double-blind, randomised, parallel-group, placebo-controlled, phase 3 trials. Lancet. 2022;399:909-923.
- Gefapixant. U.S. Food & Drug Administration Pulmonary-Allergy Drugs Advisory Committee. November 17, 2023. https://www.fda.gov/media/173927/download
- Irwin RS, Madison JM. Unexplained or refractory chronic cough in adults. N Engl J Med. 2025;392:1203-1214.
- Satia I. Management of refractory chronic cough and emerging therapies in 2025. Can Respirol Today. 2025;1:5-11. https://canadianrespirologytoday.com/article/view/1-2-Satia
- How do speech therapists treat chronic refractory cough? September 26, 2020. https://voicefit.co.uk/2020/09/26/how-do-speech-therapists-treat-chronic-refractory-cough/
- Smith JA, Birring SS, Blaiss MS, et al. Camlipixant in refractory chronic cough: a phase 2b, randomized, placebo-controlled trial (SOOTHE). Am J Respir Crit Care Med. 2025;211:1038-1048.
All URLs accessed March 23, 2026
