Diagnostic & Treatment Guidelines
Several national and international societies have developed guidelines for the workup and management of chronic cough.1,2 Clinical practice guidelines developed by the American College of Chest Physicians (ACCP), American Academy of Allergy, Asthma & Immunology (AAAAI), European Respiratory Society (ERS), American Academy of Family Physicians (AAFP), and others endorse a structured, stepwise evaluation of the underlying cause of cough, routine assessment of cough severity and cough quality of life before and after treatment, and routine follow-up within 4 to 6 weeks after the initial visit.3-7
Key guideline principles for the management of chronic cough
Treat underlying cause first1
All coughs start out as acute. The duration of cough is important to determining the likely cause, as the 8-week duration for defining chronic cough is based on research showing that post-infectious coughs due to viral, mycoplasma, or Chlamydophila infections should resolve within that timeframe. Therefore, evaluation should not be delayed once cough persists beyond 8 weeks. Clinical practice guidelines consistently stress the importance of identifying the root cause of cough in order to optimize treatment and rule out serious medical conditions.
Evaluate for common etiologies1-7
- Practice guidelines agree that the most common causes of chronic cough include upper airway cough syndrome/rhinosinus disease, asthma or eosinophilic airway disease, gastroesophageal reflux disease (GERD)/reflux, and nonasthmatic eosinophilic bronchitis.
- Evaluation of chronic cough may be detailed and time-consuming, which is challenging for many busy practitioners. However, inadequate clinical evaluation can result in premature diagnosis of “refractory chronic cough” (RCC). Chronic cough is difficult to treat when it is unexplained or fails to respond to therapy. For this reason, key elements for defining RCC are based on requirements for adequate assessment, investigation, and treatment.7
Consider hypersensitivity cough if cough is deemed truly refractory1,5,8
RCC due to neuropathic changes in vagal signaling can be more confidently diagnosed once a thorough clinical investigation has been performed according to published guidelines but no root cause has been identified. Terms such as idiopathic chronic cough, unexplained chronic cough, chronic refractory cough, difficult-to-treat cough, and cough hypersensitivity syndrome (CHS) also are used to describe this clinical condition.5,8
- Explained RCC: An underlying disorder associated with chronic cough has been identified, and coughing persists despite appropriate treatment
- Unexplained RCC: Appropriate diagnostic investigation does not indicate a root cause and there is no response to empirical therapy
Figure 1 below highlights a recommended algorithm for the comprehensive assessment of chronic cough. To foster optimal treatment selection aimed at the underlying cause, the algorithm focuses on adequate clinical evaluation of the most common causes of cough and secondary clinical evaluation of less common causes in cases of inadequate response to optimal therapy.3
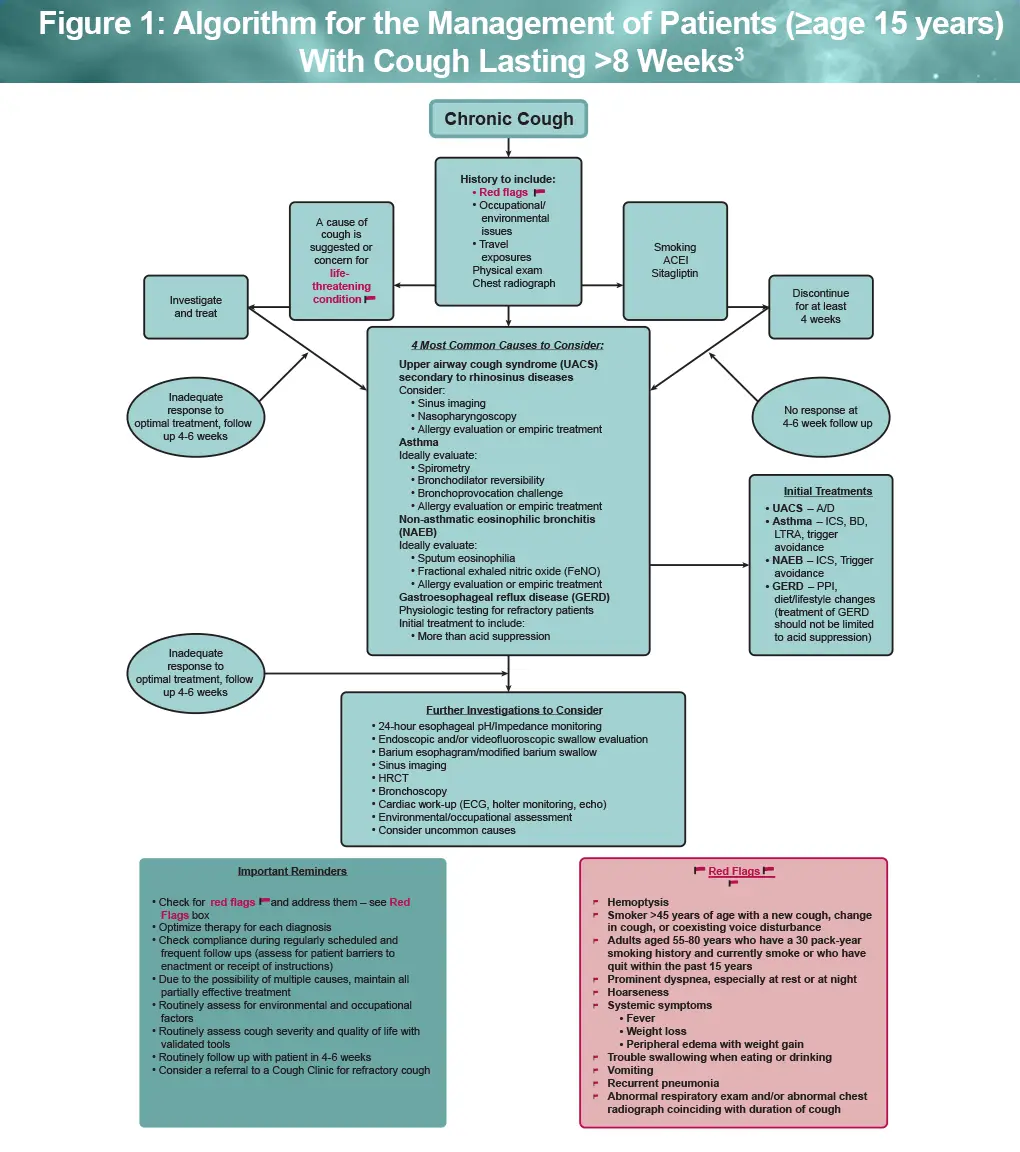
Important considerations for determining the root cause of chronic cough3:
- Be alert for red flags that indicate potentially life-threatening conditions
- Investigate for environmental and occupational exposures
- Review smoking history and medication causes, such as ACE inhibitors
- Consider potential tuberculosis infection in endemic areas and high-risk populations, even if chest X-rays are normal
- Cough due to GERD should incorporate treatment beyond acid suppression
- Assess cough severity and quality of life before and after treatment; follow up after 4 to 6 weeks
- Consider referral of patients with RCC to an interdisciplinary cough clinic
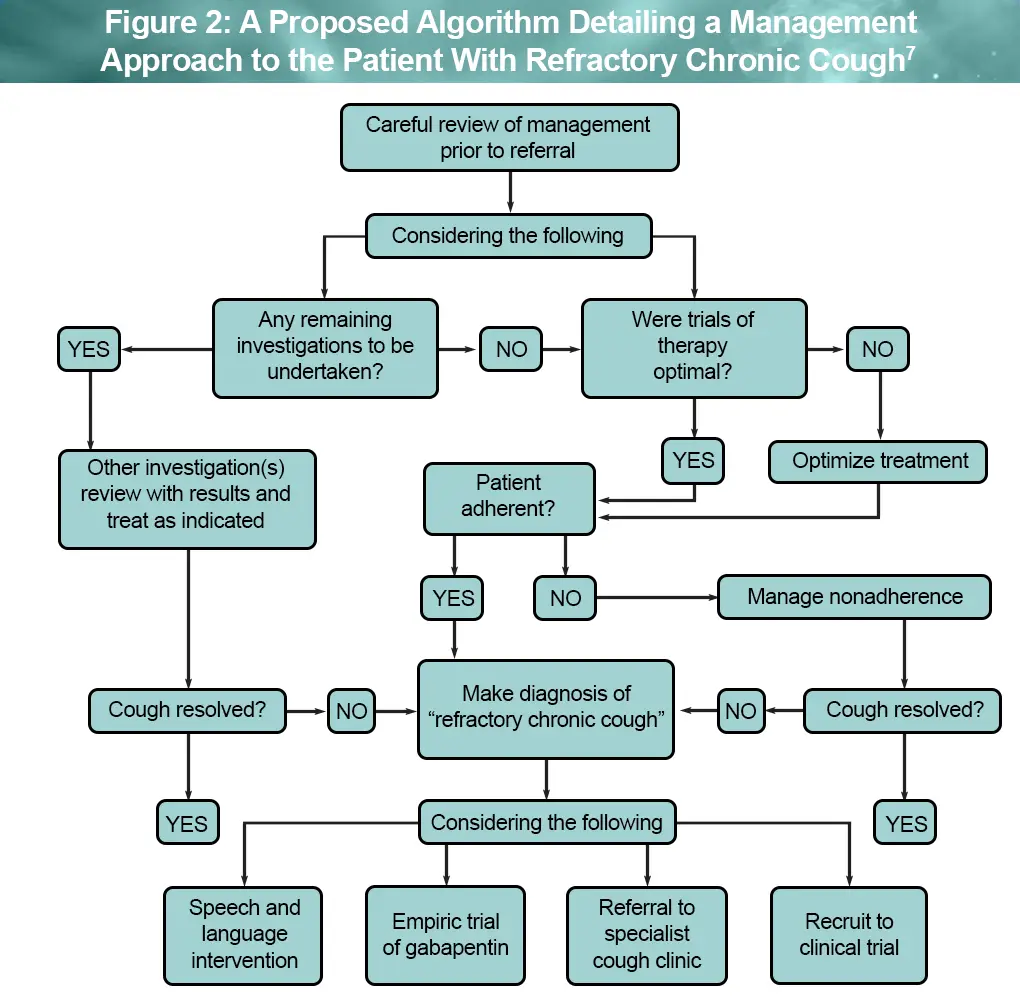
RCC is a diagnosis of exclusion. It applies to a chronic cough that persists after investigation, follow up, and therapeutic trials conducted according to published best practice guidelines in an adherent patient. The algorithm above can help with the process.
There are currently no widely approved targeted therapies specifically for RCC, and most treatments recommended in guidelines are used off-label. The ACCP and ERS suggest speech and language therapy and a trial of neuromodulator treatment, as well as clinical trial enrollment or referral to a specialized cough clinic (see Figure 2).5,7
ACEI, angiotensin-converting enzyme inhibitor; A/D, antihistamine/decongestant; BD, bronchodilator; HRCT, high-resolution CT; ICS, inhaled corticosteroid; LTRA, leukotriene antagonist; PPI, proton pump inhibitor.
Clinical practice guidelines and recommendations
- AAAAI Clinical Management Review: The Clinical Approach to Chronic Cough
- AAAI evidence-based, and expert opinion recommendations: Yardstick for managing cough, part 1
- ACCP guidelines on treatment of unexplained chronic cough
- AAFP: Chronic Cough: Evaluation and Management
- Classification of Cough as a Symptom in Adults and Management Algorithms: CHEST Guideline and Expert Panel Report
- ERS guidelines on the diagnosis and treatment of chronic cough in adults and children
- WAO-ARIA consensus on chronic cough – Part III: Management strategies in primary and cough-specialty care
References
- Irwin RS, Madison JM. Unexplained or refractory chronic cough in adults. N Engl J Med. 2025;392:1203-1214.
- Dicpinigaitis PV, Altman KW, Ulger Isci I, et al. Interdisciplinary collaboration in the diagnosis and management of chronic cough: the role and importance of primary care providers. Curr Med Res Opin. 2023;39:1375-1381.
- Irwin RS, French CL, Chang AB, et al. Classification of cough as a symptom in adults and management algorithms: CHEST Guideline and Expert Panel Report. CHEST. 2018;153:196-209.
- Irwin RS, Oppenheimer JJ, Dunlap W, et al. Yardstick for managing cough, part 1: in adults and adolescent patients older than 14 years of age. Ann Allergy Asthma Immunol. 2023;130:379-391.
- Morice AH, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur Respir J. 2020;55:1901136.
- Sonoda K, Nayak R. Chronic cough: evaluation and management. Am Fam Physician. 2024;110:167-173.
- Gibson P, Wang G, McGarvey L, et al. Treatment of unexplained chronic cough: CHEST Guideline and Expert Panel Report. CHEST. 2016;149:27-44.
- Canadian Lung Association. Breathe. Chronic cough. https://www.lung.ca/lung-health/lung-diseases/chronic-cough
All URLs accessed March 5, 2026.
