Managing Chronic Cough
Treating the root causes of chronic cough
Chronic cough remains a significant clinical challenge that markedly affects psychological, social, and physical quality of life (QoL).1-4 Recent clinical practice guidelines for diagnosis and management have focused on identifying and managing underlying disease or “treatable traits” to address the root causes of chronic cough and to guide personalized treatment.1,4
A carefully executed patient history should be conducted to identify potential underlying disease and treatable traits. Subjective and objective tools for assessing cough severity are commonly used in clinical trials but often omitted in routine practice. Assessing cough severity and its impact on QoL using simple tools (eg, QoL cough questionnaire or visual analog score) is valuable for understanding disease burden and treatment effectiveness over time.4 In addition, all patients with chronic cough require a chest X-ray, complete blood count, diagnostic spirometry, and fractional exhaled nitric oxide (FeNO).
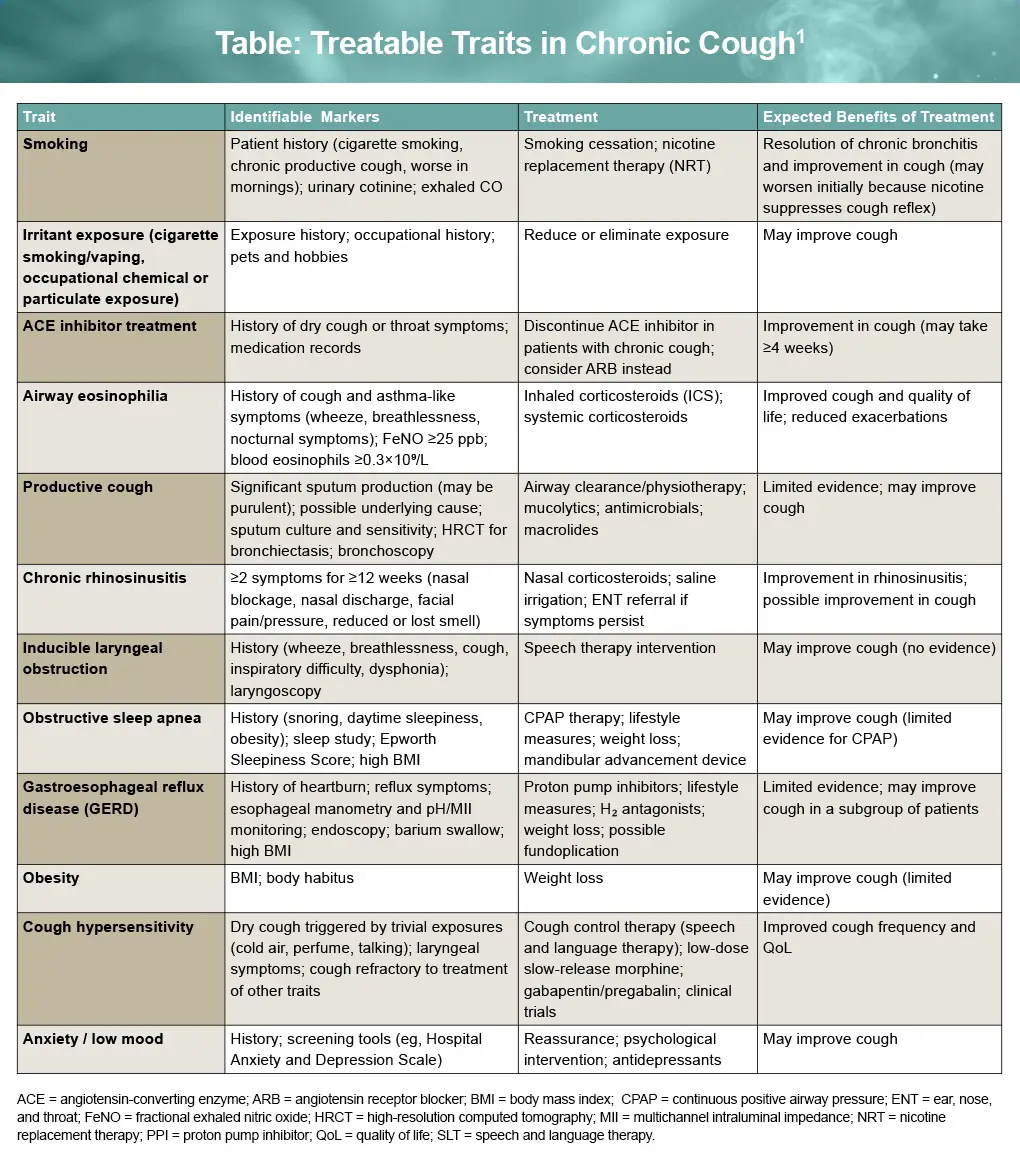
Cough hypersensitivity in refractory chronic cough (RCC) is frequently overlooked as a treatable trait and requires specific pharmacologic and nonpharmacologic treatment approaches. Table 1 outlines common treatable traits, diagnostic indicators, and corresponding treatment strategies.1
Interdisciplinary approaches to RCC management
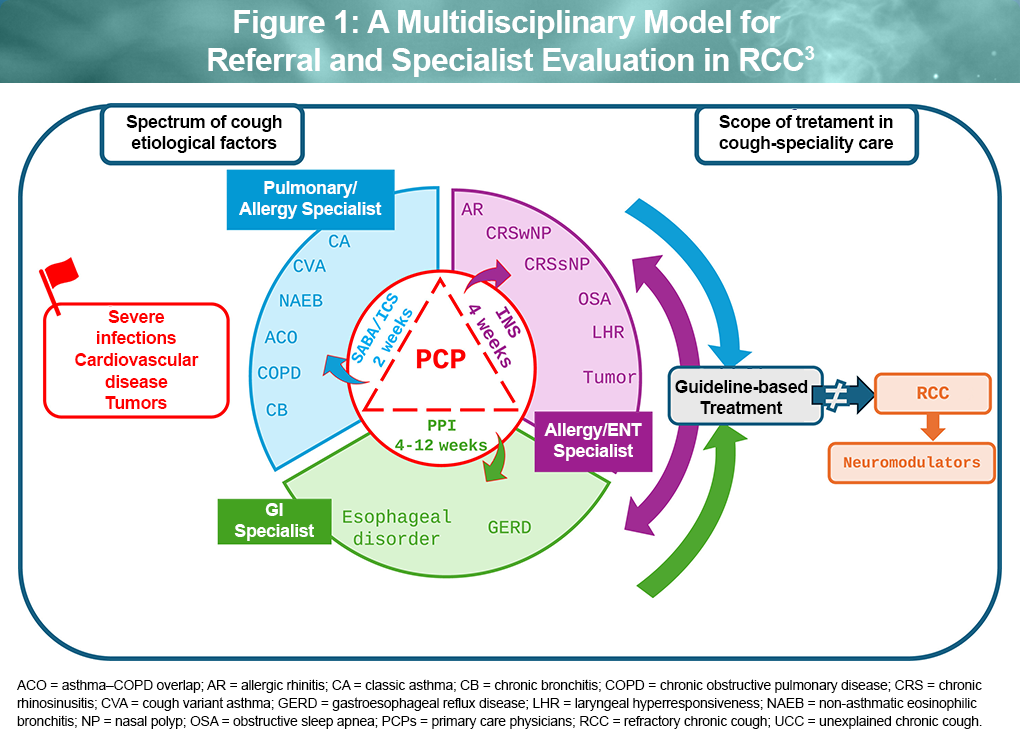
Interdisciplinary collaboration has been firmly established as a key component of optimal clinical care within complex practice settings. An important role in primary care is to determine which patients can be initially managed in general practice versus those who need referral to specialist care. ‘Red flag’ conditions such as tumors, cardiovascular disease, and severe infection require urgent referral. In addition, patients with a normal chest X-ray but no response to guideline-informed treatment for known root causes of chronic cough should be referred for secondary evaluation and treatment. The framework in Figure 1 emphasizes a multidisciplinary approach for comprehensive evaluation of RCC and management of identified treatable causes.3
Additional considerations
Urinary incontinence (UI): Chronic cough exacerbates development of stress UI, predominantly in women, and often goes untreated. Specific interventions such as pelvic physical therapy may be beneficial. Patients who suffer from UI should be referred to a urogynecologist or urologist. A clinical trial evaluating the P2X3 inhibitor gefapixant in women with UI is underway.1
Cough syncope: Although cough syncope is relatively uncommon, consequences such as potential for falls and accidents can present dangers to patients. Management focuses primarily on treating the underlying cough and reducing syncope risk. Patients who develop cough syncope should be advised not to drive.1
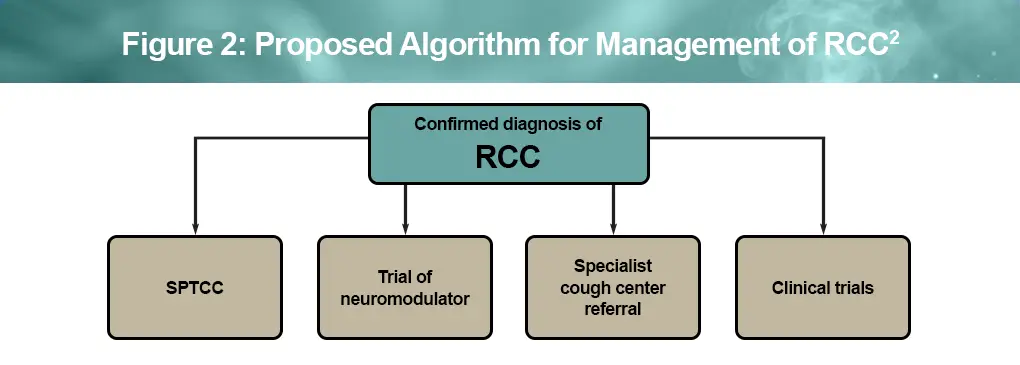
RCC is a persistent chronic cough that continues despite adequate evaluation, empiric treatment, and patient adherence to recommended therapy. Figure 2 depicts a proposed management algorithm for confirmed RCC following comprehensive, evidence-based management of chronic cough.
Nonpharmacological approaches for RCC
Speech and language therapy
RCC can persist for years with little relief from medical treatment. Speech pathology treatment for chronic cough (SPTCC) is an effective option for some patients. Although SPTCC is recommended for RCC based on clinical practice guidelines, there is no evidence-based indicator for choosing SPTCC over other therapeutic options. Therefore, symptoms, comorbidities (eg, coexisting laryngeal disorders), and patient preference should determine whether SPTCC is an appropriate next step.5
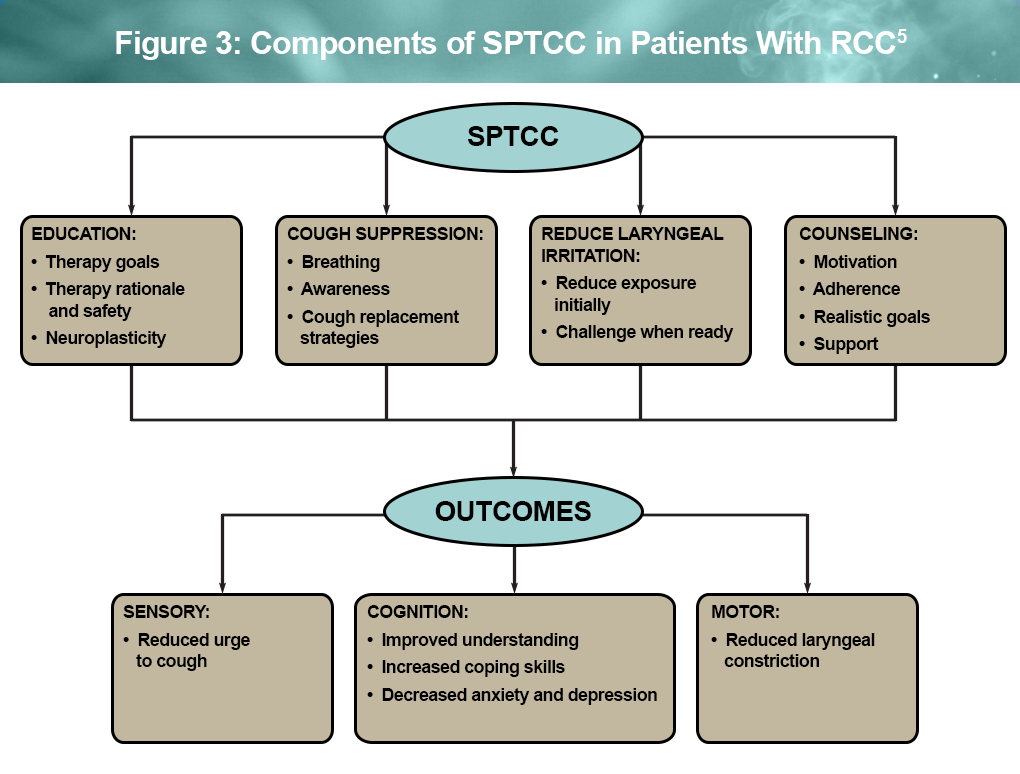
SPTCC is usually provided by a qualified speech pathologist, typically over 3 to 4 sessions, and is associated with reduced cough hypersensitivity, urge to cough, and cough frequency as well as improved QoL. Although the exact mechanism of benefit is not fully understood, evidence suggests that speech pathology may lessen cough reflex sensitivity and enhance cortical control of cough. Components of SPTCC include education, cough suppression, reduction in laryngeal irritation, and counselling, with the objectives of reducing cough hypersensitivity and improving cognitive skills and motor function as outlined in Figure 3 below.5
Lifestyle modification
Several lifestyle modifications may be helpful to reduce symptoms of RCC, including environmental, dietary, and physical approaches. These interventions should be individualized based on patient tolerance, underlying etiologies, and comorbidities.6,7
Avoidance of irritants6,7
Reducing exposure to airway irritants may help minimize cough triggers and airway inflammation:
- Smoking cessation and avoidance of secondhand smoke
- Minimizing exposure to environmental irritants such as chemical fumes, pollutants, pollen, and molds
- Avoiding occupational exposures known to trigger cough when possible
Dietary modifications7-9
Dietary strategies can be helpful, particularly in patients with GERD-associated cough or laryngopharyngeal reflux:
- Avoid foods and beverages that may trigger cough or reflux, including spicy foods, acidic foods, and cold beverages
- High caloric and high-fat intake has been associated with greater cough severity
- Recommend an anti-reflux diet, such as a high-protein, plant-based, alkaline diet with lower sugar content
- Eat smaller portion sizes and avoid large meals, especially at night
- Avoid eating within 2 hours of bedtime
Patients may benefit from nutritional counseling, particularly when cough is associated with environmental or occupational exposures. An anti-inflammatory, low-glycemic, nutrient-dense diet and targeted nutraceutical supplementation may support detoxification, augment gut health, and improve gastrointestinal function when implemented under supervision of a registered dietitian in collaboration with the treating clinician.9
Hydration and airway moisturization6
Maintaining adequate hydration can help keep the throat moist and reduce irritation:
- Maintain adequate daily hydration (≥1.5 L/day) to facilitate mucus clearance
- Steam inhalation or a cool-mist humidifier can hydrate airway passages
- Soothe throat irritation with lozenges, hard candy, or honey
Physical activity and breathing techniques6,7
Regular physical activity and breathing exercises may improve respiratory function and cough control:
- Moderate-intensity aerobic exercise (eg, swimming, Tai Chi) may improve lung function
- Respiratory training techniques such as pursed-lip breathing and diaphragmatic breathing may improve cough control
- Airway clearance techniques, including postural drainage or ultrasonic nebulization, may facilitate sputum clearance
Comorbid anxiety and depression
RCC is strongly associated with anxiety and depression, and psychological factors may both contribute to and arise from persistent cough. This bidirectional relationship may reflect the effects of RCC on sleep, social functioning, and overall QoL.¹⁰
In general, patients with RCC report higher levels of fatigue, somatic symptoms, depression, and anxiety than those without chronic cough. In addition, patients with unexplained RCC often report reduced illness coherence and greater distress, with heightened attention to cough sensations that potentially perpetuates the cycle of persistent coughing.¹¹
Patients with anxiety or depression diagnosed prior to the onset of RCC report greater symptom severity than those without a prior mental health diagnosis, underscoring the need for holistic care in patients with RCC.¹²
Overall, RCC involves a complex relationship between cough and psychological distress. Thus, addressing psychological factors, including with pharmacologic approaches such as amitriptyline—a tricyclic antidepressant — may help reduce cough severity.¹⁰
References
Parker SM, Smith JA, Birring SS, et al. British Thoracic Society Clinical Statement on chronic cough in adults. Thorax. 2023;78(suppl 6):s3-s19.
Gibson P, Wang G, McGarvey L, et al. Treatment of unexplained chronic cough: CHEST Guideline and Expert Panel Report. CHEST. 2016;149:27-44.
Rouadi PW, Idriss SA, Bousquet J, et al. WAO – ARIA consensus on chronic cough: executive summary. World Allergy Organ J. 2025;18:101034.
Satia I, Hassan W, McGarvey L, et al. The clinical approach to chronic cough. J Allergy Clin Immunol Pract. 2025;13:454-466.
Vertigan AE, Haines J, Slovarp L. An update on speech pathology management of chronic refractory cough. J Allergy Clin Immunol Pract. 2019;7:1756-1761.
Hu X, Zhang K, Liu T, et al. Chronic cough: a review and prospects. Medicine (Baltimore). 2025;104:e45162.
Canadian Lung Association. Breathe. Chronic cough. https://www.lung.ca/lung-health/lung-diseases/chronic-cough
Hránková V, Balner T, Kondé A, et al. The role of an anti-reflux diet in the treatment of chronic cough caused by laryngopharyngeal reflux. Eur Arch Otorhinolaryngol. 2025;282:2009-2013.
Bergman N, Riley DS, Beidelschies M. Diet and lifestyle recommendations for the treatment of chronic cough and chronic disease. BMJ Case Rep. 2018;2018:1-5.
Irwin RS, Madison JM. Unexplained or refractory chronic cough in adults. N Engl J Med. 2025;392:1203-1214.
Hulme K, Deary V, Dogan S, et al. Psychological profile of individuals presenting with chronic cough. ERJ Open Res. 2017;3:00099-2016.
Hari G, Naunheim M, Kallogjeri D, et al. Anxiety and depression diagnoses and the Cough Severity Index: a retrospective study. Ear Nose Throat J. 2026;105:23-28.
All URLs accessed April 13, 2026
