Pathophysiology
Most cases of chronic cough are benign and resolve with appropriate clinical evaluation and treatment. However, refractory chronic cough (RCC) persists despite optimal management, and may be idiopathic. Although the term unexplained chronic cough (UCC) is often used in clinical trials to stratify patients, it is used less often in clinical practice because it may be perceived as dismissive or invalidating, implying that the cough has no underlying pathology. RCC and UCC have also been described as cough hypersensitivity syndrome (CHS), highlighting the need for more consistent nomenclature.1
Etiologies of chronic cough in adults
Etiologies of chronic cough are broadly classified by anatomical origins involving the upper airway, lower airway, or gastroesophageal mechanisms. Additionally, comorbid pathologies include laryngeal hyperresponsiveness, obstructive sleep apnea, angiotensin converting enzyme (ACE) inhibitor-induced cough, post─COVID-19 cough, psychological cough, and multifactorial cough. The various phenotypes of chronic cough are listed in the Table.2,3
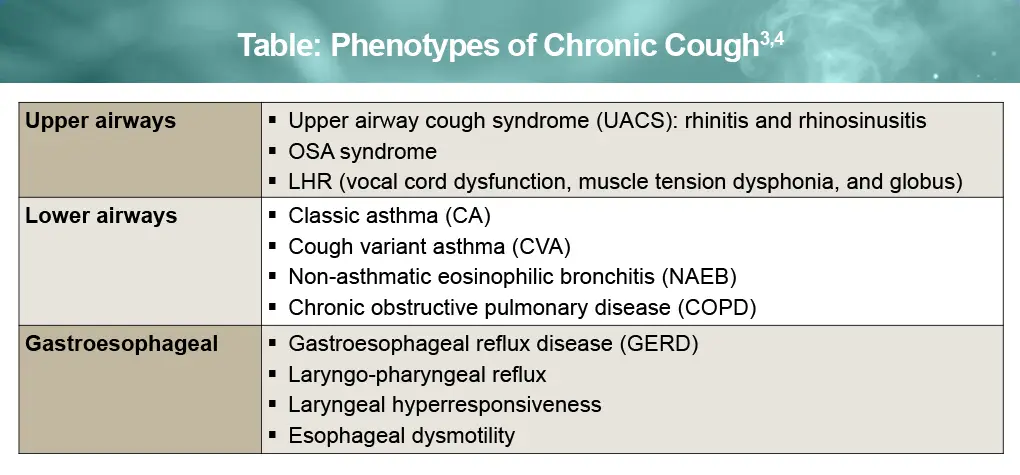
Severe persistent multifactorial cough is not well-characterized in terms of prevalence, symptoms, and response to therapy. The most common underlying cough phenotype in adults is atopic cough with GERD. GERD-associated cough in combination with either upper or lower airway etiologies is typically more severe than airway-only phenotypes.3,4
Neuroanatomy and physiology of RCC
Although many chronic cough cases can be attributed to identifiable etiologies, persistent cough may also reflect dysregulation of the cough reflex itself. Understanding the neuroanatomy and physiology of the cough reflex helps explain the mechanisms underlying cough hypersensitivity and RCC.
Coughing is a neuronal defensive reflex designed to protect the airways from thermal, mechanical, and chemical damage. Hypertussia may be triggered by talking, laughing, singing, or exposure to temperature changes, strong odors, and aerosol chemicals. Increasingly, it’s been recognized that stimulation of vagal afferents that innervate the larynx, trachea, and large airways transmit signals through the jugular and nodose ganglia to the brainstem cough center in the nucleus tractus solitarius (nTS), initiating the cough reflex.1
Numerous studies of cough hypersensitivity involving an inhalation challenge (eg, with capsaicin), have demonstrated dysregulated neuronal reflex in patients with RCC. It is thought that the cough reflex undergoes both neurogenic and inflammatory alterations in the vagal neuronal pathways and thus becomes hyperresponsive. However, the source of neuronal hypersensitivity is unclear in any given patient, as it may reflect peripheral sensitization, central sensitization, and/or impaired descending inhibitory control mechanisms, similar to those associated with chronic pain.1-3
Modulation of the cough reflex is thought to involve multiple neuromediators, including neurokinin, bradykinin, prostaglandins, and calcitonin gene-related peptide, as well as activation of immune cells such as mast cells, eosinophils, and neutrophils. P2X3 receptors and transient receptor potential (TRP) channels expressed on vagal afferent fibers (ie, Aδ and C fibers) play a key role in detecting airway irritants and adenosine triphosphate released during epithelial injury.5,6 Activation of P2X3 and TRP receptors contributes to neuro-immune crosstalk, lowering the neuronal cough threshold and leading to cough hypersensitivity, as depicted in Figure 1.3
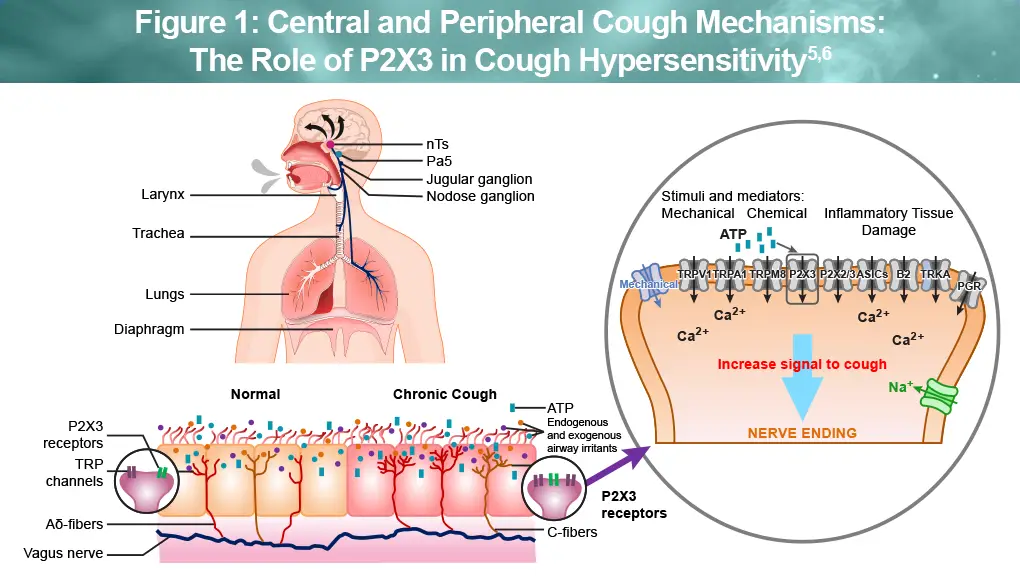
ATP, adenosine triphosphate; NK-1, neurokinin-1 receptor; nTS, nucleus of the solitary tract; Pa5, paratrigeminal nucleus; TRPV1, TRP vanilloid-1.
Neurologic, psychological, or psychogenic causes of coughing6
Although uncommon, certain neuropsychological and behavioral disorders may contribute to chronic cough in adults. These conditions are rare compared with more common medical etiologies of cough. Careful evaluation and use of terminology defined by the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, are helpful to avoid misdiagnosis and inappropriate labeling of patients.
- Somatic cough syndrome (previously called psychogenic cough)
- Tic cough (motor and phonic) due to recurrence of Tourette’s syndrome diagnosed in childhood
Because all patients with unresolved chronic cough are at risk for psychological symptoms, it’s important to avoid automatic assumptions that the underlying cause of RCC is anxiety, depression, or other neuropsychological condition. In fact, anxiety and depression often resolve with disappearance of cough symptoms.
References
- Satia I. Management of refractory chronic cough and emerging therapies in 2025. Can Respirol Today. 2025;1:5-11. https://canadianrespirologytoday.com/article/view/1-2-Satia
- Smith JA, Satia I, Badri H, et al. Mini-review: hypertussivity and allotussivity in chronic cough endotypes. Neurosci Lett. 2023;792:136934.
- Rouadi PW, Idriss SA, Bousquet J, et al. WAO – ARIA consensus on chronic cough: executive summary. World Allergy Organ J. 2025;18:101034.
- Smith JA, Houghton LA. The oesophagus and cough: laryngo-pharyngeal reflux, microaspiration and vagal reflexes. Cough. 2013;9:12.
- Drake MG, McGarvey LP, Morice AH. From bench to bedside: the role of cough hypersensitivity in chronic cough. Clin Transl Med. 2023;13:e1343.
- Irwin RS, Madison JM. Unexplained or refractory chronic cough in adults. N Engl J Med. 2025;392:1203-1214.
All URLs accessed April 13, 2026
