Challenges of Chronic Cough
Disease burden of chronic cough
Cough is one of the leading causes for physician visits worldwide.1 Results of a survey in 2018 by the Ambulatory and Hospital Care Statistics Branch at the National Center for Health Statistics showed that 2.1% of the total 860,386 visits to ambulatory care providers in the United States were due to cough, putting it in the top 10 reasons for medical visits.2
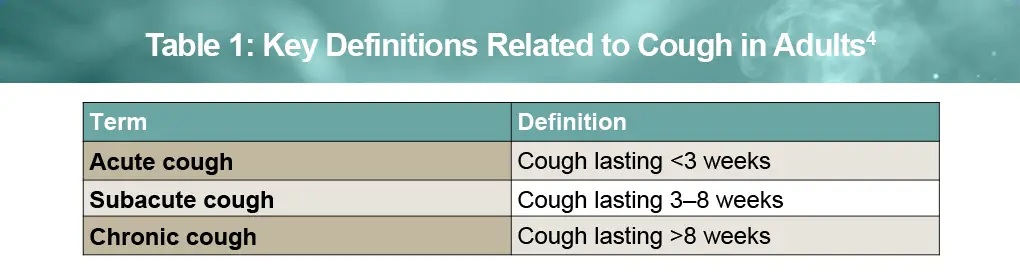
Chronic cough is defined by the American College of Chest Physicians (CHEST) as one that lasts beyond a duration of 8 weeks, whereas acute cough lasts <3 weeks (see Table 1).3 Chronic cough affects ~5% of US adults and is more prevalent in women than men.4 Other risk factors include older age, lower educational attainment, and comorbidities such as chronic obstructive pulmonary disease, chronic sinusitis, bronchiectasis, pulmonary fibrosis, hypertension, depression, and cough-related complications.5
The impact of chronic cough on quality of life
The journey to diagnosis and treatment for patients with chronic cough, based on symptoms and the potential root cause, can be very different from one patient to another. For example, although chronic cough is defined as one lasting for more than 8 weeks, many patients suffer from chronic cough lasting for years despite multiple clinic visits involving multiple diagnostic evaluations and treatments.4
The frequency of chronic cough can range from fewer than 10 coughs per day to 100 coughs per hour. Regardless of the underlying cause, chronic cough has a significant impact on daily activities and may lead to anxiety, depression, symptoms such as incontinence, syncope/fainting, broken ribs, chest pain, and hoarseness, as well as reduced quality of life and ability to work and engage in social situations. For these reasons, greater awareness and better management of chronic cough are needed throughout all levels of healthcare, and particularly for primary care providers (PCPs) who have the greatest opportunity to ensure an appropriate clinical workup and timely diagnosis for patients seeking treatment.4
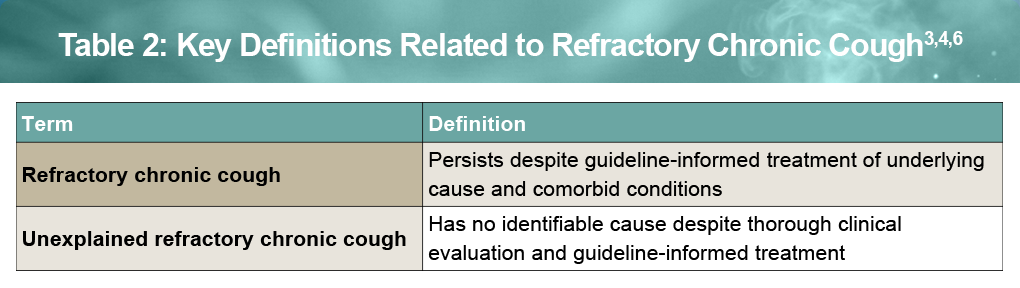
According to CHEST guidelines, cough duration is an important early step in evaluating likely causes, particularly beyond the 8-week mark. Increasing evidence suggests that chronic cough may represent a distinct disease entity. While treatment of common associated conditions such as upper airway cough syndrome, asthma, and gastroesophageal reflux disease can resolve chronic cough, many patients have cough that persists despite appropriate evaluation and guideline-based management. This scenario is defined as refractory chronic cough (RCC; see Table 2) and, despite extensive investigation, there may be no explainable treatable cause.5 Incidence rates as high as 60% have been reported for adults with unexplained or RCC; however, in a rigorous systematic review the prevalence was closer to 10%.6
Clinical challenges and unmet needs in RCC
Although RCC is a burdensome condition that can significantly impact daily living, patients often undergo multiple diagnostic evaluations and treatment trials before refractory chronic cough is recognized (see Figure).4

In one comprehensive survey-based study of 565 patients with documented high degree of cough burden, the average duration of cough was 8.6 years, with an average weekly severity score of 5.3/10, and treatment responses were characterized as suboptimal.8
There are currently no FDA-approved therapies for RCC. Recommended therapies included in clinical practice guidelines are generally used off-label and yield inadequate responses for many patients.7 In addition, a Cochrane meta-analysis found no evidence supporting the effectiveness of over-the-counter medications for acute cough and noted that these therapies have not been studied in chronic cough.9
Consequently, RCC remains a substantial unmet clinical need, highlighting the urgency for timely diagnosis and effective, evidence-based therapies to improve patient outcomes and QoL.10
References
- Finley CR, Chan DS, Garrison S, et al. What are the most common conditions in primary care? Systematic review. Can Fam Physician. 2018;64:832-840.
- Santo L, Okeyode T. National Ambulatory Medical Care Survey: 2018 National Summary Tables. US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics. https://www.cdc.gov/nchs/data/ahcd/namcs_summary/2018-namcs-web-tables-508.pdf
- Gibson P, Wang G, McGarvey L, et al. Treatment of unexplained chronic cough: CHEST Guideline and Expert Panel Report. CHEST. 2016;149:27-44.
- Dicpinigaitis PV, Altman KW, Ulger Isci I, et al. Interdisciplinary collaboration in the diagnosis and management of chronic cough: the role and importance of primary care providers. Curr Med Res Opin. 2023;39:1375-1381.
- Zeiger RS, Schatz M, Zhou Y, et al. Risk Factors for persistent chronic cough during consecutive years: a retrospective database analysis. J Allergy Clin Immunol Pract. 2022;10:1587-1597.
- Irwin RS, French CL, Chang AB, et al. Classification of cough as a symptom in adults and management algorithms: CHEST Guideline and Expert Panel Report. CHEST. 2018;153:196-209.
- Refractory chronic cough (RCC) therapeutics. Pipeline analysis & competitive landscape 2026-2035. December 2025. https://support.hyfe.com/hubfs/Hyfe%20White%20Papers/Chronic%20Cough%20Treatment%20-%20Pipeline%20Analysis%20and%20Competitive%20Landscape%202026%20-%202035.pdf Accessed March 6, 2026.
- Zeiger RS, Schatz M, Hong B, et al. Patient-reported burden of chronic cough in a managed care organization. J Allergy Clin Immunol Pract. 2021;9:1624-1637.e10.
- Smith SM, Schroeder K, Fahey T. Over-the-counter (OTC) medications for acute cough in children and adults in community settings. Cochrane Database Syst Rev. 2014 Nov 24;2014(11):CD001831.
- Satia I, Wahab M, Kum E, et al. Chronic cough: investigations, management, current and future treatments. Can J Resp Crit Care Sleep Med. 2021;5:404-416.
URLs accessed April 13, 2026
