Diagnosis
Patients with chronic cough (CC) often experience symptoms for years, frequently use healthcare resources, undergo multiple treatment trials that may be unsuccessful, and still may not receive a clear explanation for the cause of their cough. Because CC can be associated with a wide range of underlying conditions, identifying contributors can be diagnostically challenging and may require multidisciplinary involvement. In addition, clinical practice guidelines do not clearly define the role of primary care providers (PCPs) in evaluating and managing CC, including refractory chronic cough (RCC).
Yet PCPs play an important role in the diagnosis and management of CC, particularly during the initial evaluation and treatment of common causes. A thorough primary care workup may help identify the cause or causes of cough earlier and support a more efficient path to appropriate management.1
Clinical signs and symptoms
According to clinical practice guidelines from the American College of Chest Physicians, European Respiratory Society, and others, initial assessment for CC includes a detailed history and thorough physical examination, as well as a chest X-ray, to identify specific causes due to underlying disease exposures (occupational, environmental, travel). Red-flag signs and symptoms of potentially serious underlying disease include hemoptysis, prominent dyspnea at rest, significant productive cough, and recurrent pneumonia. Spirometry, ideally combined with bronchodilator testing, should be performed in all patients to assess for asthma and chronic obstructive pulmonary disease (COPD). 1-4
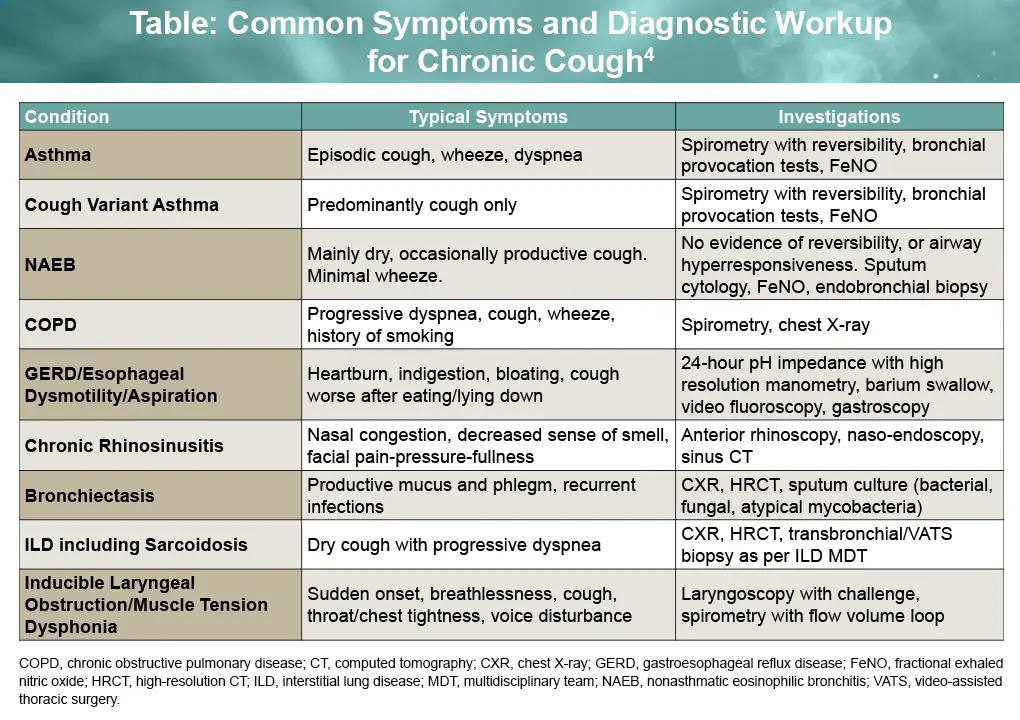
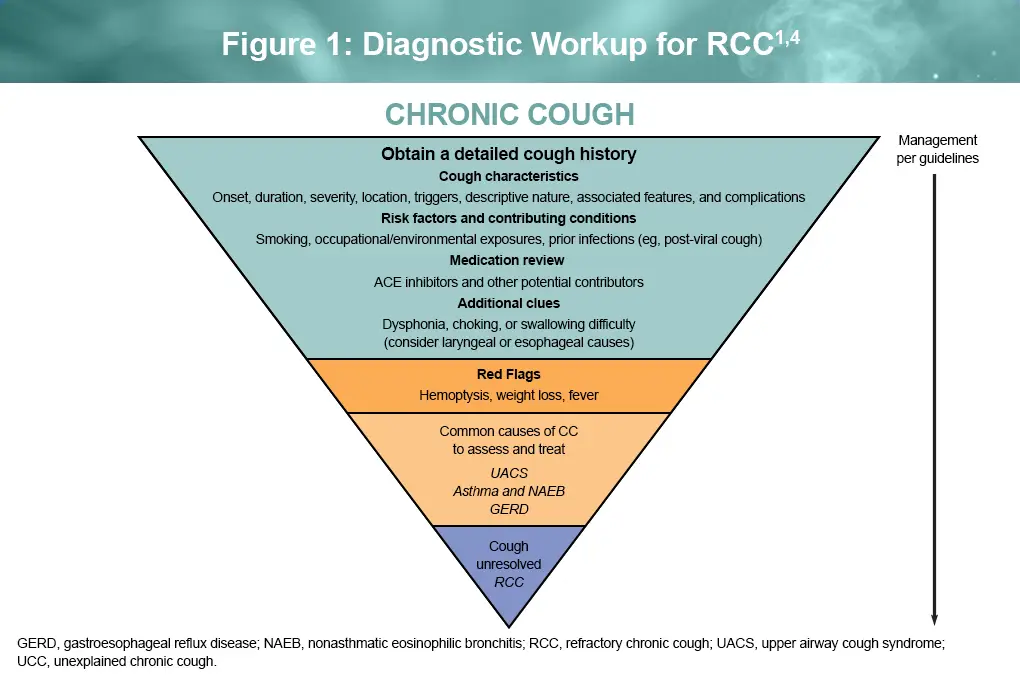
However, many patients don’t seek medical care for their cough or mention it to their PCP. In one study, 60% of patients >64 years of age had not sought medical evaluation for an existing cough. Importantly, PCPs should obtain a detailed cough history and should specifically ask about cough onset, duration, severity, triggers, nature, and location, as well as prior infections, which commonly cause acute cough.1,4 Patients with CC often report that their cough began with an acute viral upper respiratory tract infection. In addition, medication history, including use of angiotensin converting enzyme (ACE)-inhibitors should be assessed.1,4
Further evaluation should be guided by presenting symptoms, with consideration of the most common causes of CC1-3:
- Upper-airway cough syndrome (UACS)
- Asthma
- Nonasthmatic eosinophilic bronchitis (NAEB)
- Gastroesophageal reflux disease (GERD)
Patients often report symptoms of UACS (rhinorrhea, nasal congestion, and postnasal drip), asthma (wheezing, dyspnea, chest tightness), or GERD. If cough resolves after recommended treatment of a suspected underlying condition, the condition is presumed to have been a contributing cause of the cough.1,2 Figure 1 outlines a guideline-based diagnostic approach to chronic cough, beginning with initial assessment, including a focused cough history, and progressing through evaluation of common causes.
Differential diagnosis
Referral should be considered for patients whose chronic cough does not respond to treatment, particularly when red-flag symptoms are present or when lung cancer, bronchiectasis, interstitial lung disease, heart failure, or tuberculosis is suspected. Referral may also be appropriate for further testing (eg, computed tomography or bronchoscopy) and for management with off-label neuromodulators (eg, gabapentin, pregabalin) or speech therapy.4
Collaboration between primary care providers and specialists, including pulmonologists, allergists, otolaryngologists, and gastroenterologists, can help to optimize chronic cough care and reduce patient burden through more timely diagnosis and effective management.5
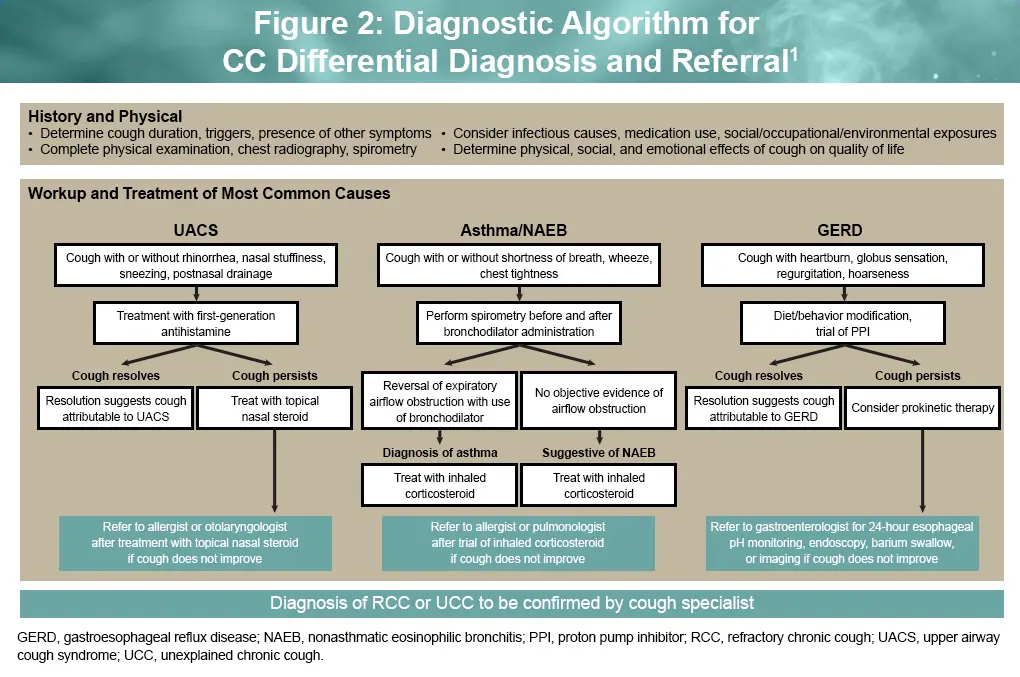
According to the World Allergy Organization Allergic Rhinitis and Impact on Asthma consensus statement, primary evaluation by PCPs should focus on history-taking, comprehensive physical examination, and chest X-ray to identify cough-related triggers, risk factors (ie, smoking, environmental/occupational exposure), and other common causes (eg, ACE inhibitors, infections), including appropriate evaluation and management of upper- and lower-airway disease and GERD. Patients with cough that persists after treatment of common comorbid conditions (ie, UACS, asthma, NAEB, GERD) should be referred to a specialist.5 However, in one study of 235,457 electronic health records of patients with cough, only 23% had a cough-related diagnostic code or received medication and only 3.0% were referred for specialist care (pulmonologists, 64%; otolaryngologists, 29%; allergists, 5%; gastroenterologists, 4%), highlighting opportunities for stronger PCP-specialist partnership to improve diagnosis and management of patients with chronic cough (Figure 2).1,6
Diagnostic workup and secondary evaluation of RCC
While many patients improve with treatment of common causes, a subset continues to experience persistent cough despite appropriate evaluation and management. RCC may be diagnosed when cough persists despite appropriate diagnostic workup and guideline-directed management. In some patients, no associated condition is identified despite a thorough workup, resulting in a diagnosis of unexplained RCC. Note that the presence of a comorbid condition does not necessarily mean that the condition is causing the cough. Conditions such as UACS, asthma, and GERD are common in patients with chronic cough, but treating them does not always lead to cough resolution. In recent phase 3 trials of patients with RCC, 60% had prior diagnoses, most often with UACS, asthma, and/or GERD, whereas the remaining 40% had unexplained RCC. RCC reflects a state of cough hypersensitivity in which otherwise mild stimuli can provoke an exaggerated cough response. The same comorbid conditions may not trigger chronic cough in individuals without heightened cough sensitivity. Symptoms may include persistent tickling, irritation, or a raw sensation in the throat or laryngeal area, allotussia (cough triggered by innocuous stimuli such as talking or laughing), and hypertussia (an exaggerated cough response to typical stimuli).4
Diagnostic delays and healthcare burden in RCC
Delayed recognition of RCC has implications for both patients and for healthcare utilization. Limited use of efficient diagnostic strategies for RCC, together with gaps in understanding of its etiology and pathophysiology, can delay diagnosis and treatment. Unfortunately, these challenges contribute to inconsistent representation of RCC in diagnostic and management guidelines. In an observational study of 200 patients with RCC, patients suffered an average of 8 years before receiving an RCC diagnosis, at significant cost to themselves and the health care system. In the 5 years before receiving an RCC diagnosis at a specialist cough clinic, patients with RCC had 3-fold higher healthcare resource utilization than matched controls. Although those costs declined after diagnosis, they remained higher than those of controls for months to years afterward. These findings underscore the need for more efficient referral pathways to specialist evaluation and for novel therapies that target the underlying mechanisms of cough hypersensitivity in RCC.7
References
- Dicpinigaitis PV, Altman KW, Ulger Isci I, et al. Interdisciplinary collaboration in the diagnosis and management of chronic cough: the role and importance of primary care providers. Curr Med Res Opin. 2023;39:1375-1381.
- Gibson P, Wang G, McGarvey L, et al. Treatment of unexplained chronic cough: CHEST Guideline and Expert Panel Report. CHEST. 2016;149:27-44.
- Morice AH, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur Respir J. 2020;55:1901136.
- Satia I, Wahab M, Kum E, et al. Chronic cough: investigations, management, current and future treatments. Can J Resp Crit Care Sleep Med. 2021;5:404-416.
- Rouadi PW, Idriss SA, Bousquet J, et al. WAO-ARIA consensus on chronic cough–part III: management strategies in primary and cough-specialty care. Updates in COVID-19. World Allergy Organ J. 2022;15:100649.
- Weiner M, Dexter PR, Heithoff K, et al. Identifying and characterizing a chronic cough cohort through electronic health records. Chest. 2021;159:2346-2355.
- Smith JA, Stein N, Migas S, et al. An observational study to understand burden and cost of care in adults diagnosed with refractory chronic cough (RCC) or unexplained chronic cough (UCC). Respir Res. 2024;25:265.
All URLs accessed April 13, 2026
