Pharmacologic Treatment for RCC
Management of chronic cough involves a stepwise approach that begins with identifying and treating underlying disease or treatable traits. Often, cough can be caused by more than one common condition, such as asthma, NAEB, UACS, or GERD. For all of these conditions, a focused trial of therapy is appropriate.1-4
Secondary evaluation of RCC
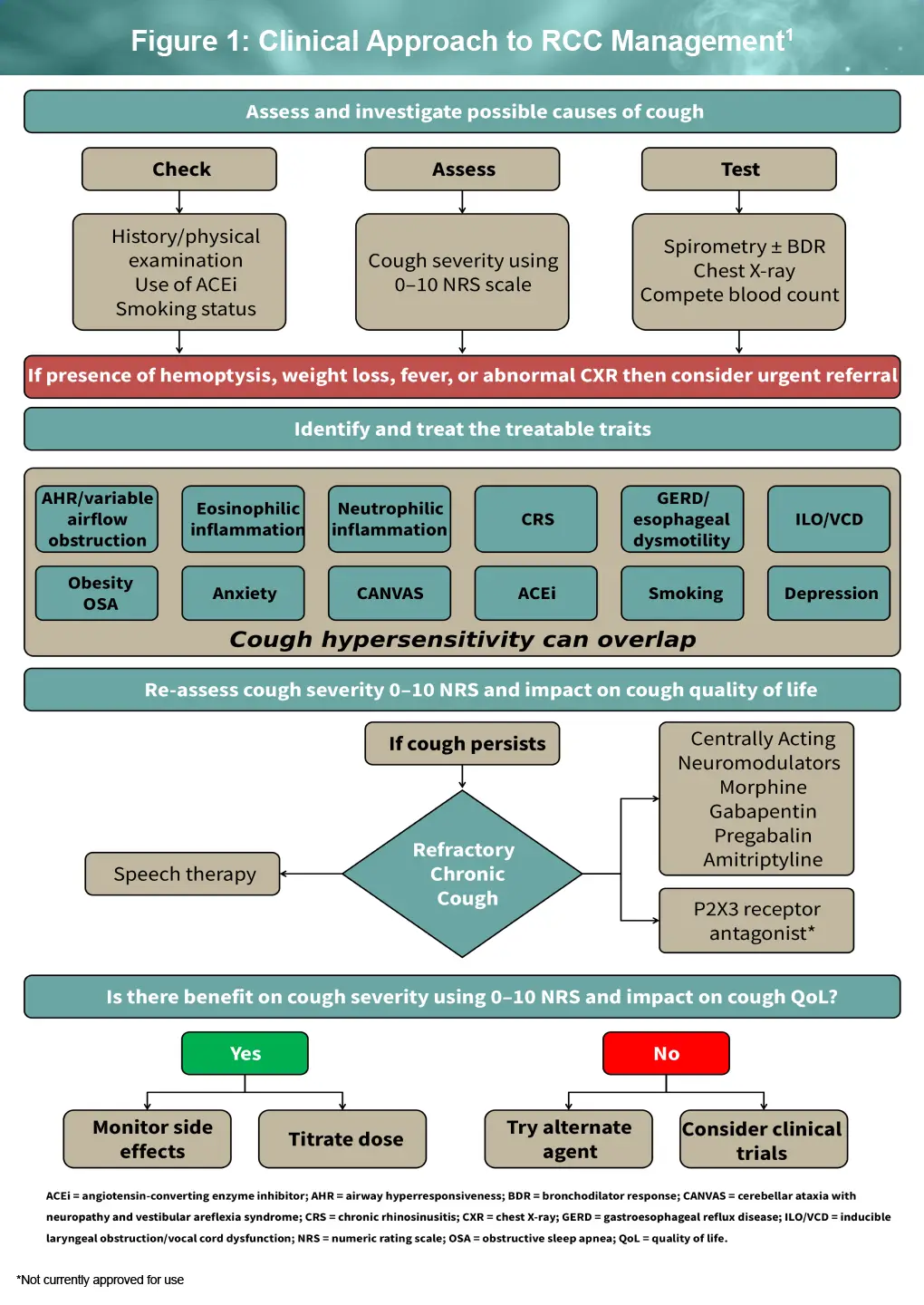
Chronic cough may be associated with treatable traits and overlapping cough hypersensitivity, even early in the disease course. Therefore, routine evaluation of cough severity and effect on quality of life (QoL) is recommended. The overlapping nature of treatable traits and cough hypersensitivity highlights the multifactorial etiology of RCC, and the importance of identifying and managing underlying conditions to inform a comprehensive treatment plan. Figure 1 below emphasizes regular assessment of cough severity and cough-related QoL as part of RCC management 1
Pharmacologic therapies for RCC1
Centrally acting neuromodulators: Neuromodulators for RCC include low-dose morphine, gabapentin, and pregabalin, all of which have demonstrated improvement of symptoms and QoL in small randomized clinical trials. However, at the doses evaluated in clinical trials, all of these agents were associated with adverse events (AEs), including dizziness, drowsiness, and fatigue.
- Gabapentinoids: A trial of gabapentin or pregabalin should be cautiously titrated up to the lowest effective dose, as these agents are associated with abuse and addiction. Gabapentin is typically started at a dose of 100 mg t.i.d. and titrated up to 600 mg t.i.d.
- Low-dose morphine: A 2-week trial of low-dose morphine (5 to 10 mg) can be started after a discussion with the patient regarding the risks and benefits of opioid therapies. The benefit will be apparent within 5 days in most patients who are likely to have a response
- Amitriptyline 10 mg at bedtime was evaluated in an unblinded study and demonstrated reported symptomatic improvement
- Baclofen, a peripheral and central γ-aminobutyric acid type β agonist, was found to be of limited practical value due to side effects and tolerability
Notably, there is no documented evidence that cough suppression leads to serious AEs due to impaired mucus clearance in patients with RCC who have normal spirometry and normal chest imaging.
Emerging Therapies for RCC
After decades of limited treatment choices for RCC, several novel agents are currently in development, primarily targeting peripheral sensory pathways involved in cough hypersensitivity.
P2X3 antagonists
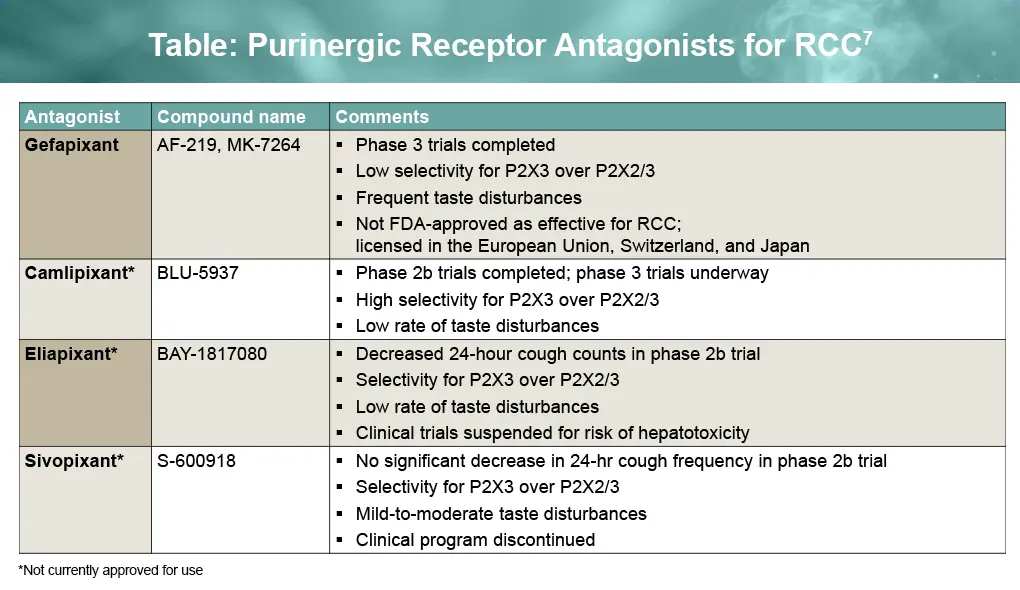
Oral purinergic antagonists are designed to block P2X3 and P2X2/3 receptors on vagal afferent nerves. Gefapixant is the only P2X3 antagonist to have received regulatory approval, and it did so outside the United States; no purinergic antagonists are approved by the FDA for RCC, but this drug class has shown promise in RCC. Among the agents studied so far, camlipixant appears to offer one of the most favorable profiles for safety and efficacy. The Table below summarizes purinergic antagonists with varying selectivity for P2X3 and P2X2/3 receptors that have been studied in phase 2 or later clinical trials.5,6
Gefapixant 5,6,8
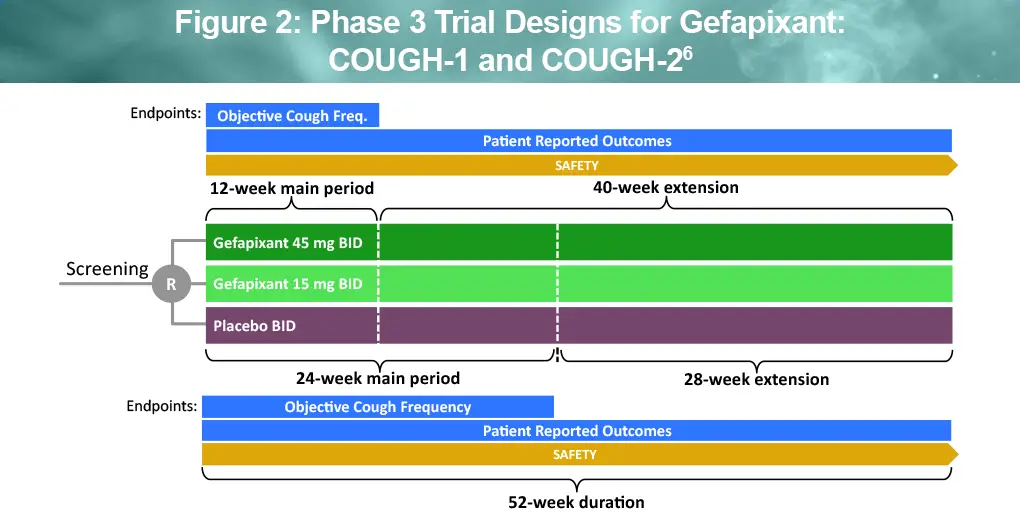
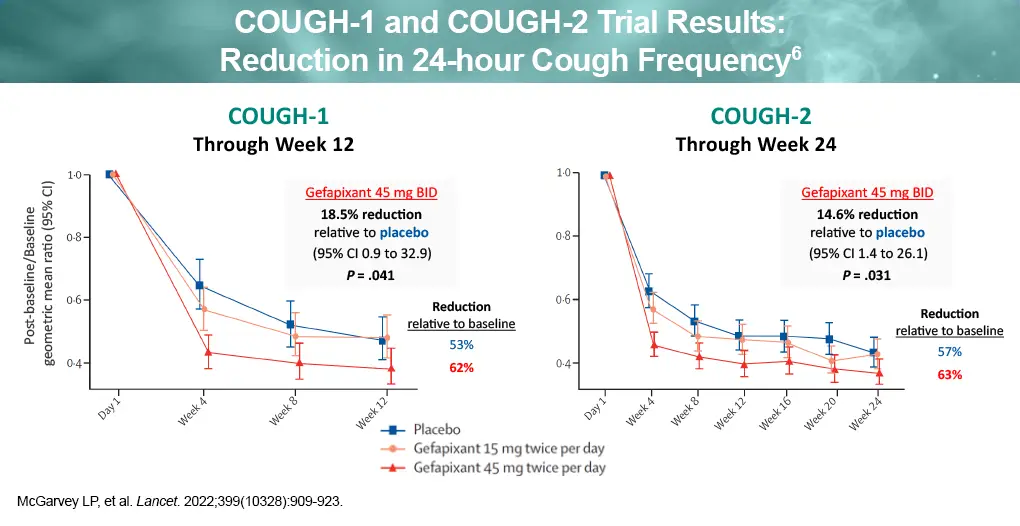
Gefapixant was evaluated in two phase 3 randomized clinical trials, COUGH-1 and COUGH-2, which showed modest efficacy (see Figure 2). Patients with RCC or unexplained chronic cough (UCC) of ≥1 year duration and cough severity visual analogue scale score of ≥40 mm were randomized to oral gefapixant 15 mg twice daily, gefapixant 45 mg twice daily, or placebo. Results in the 45-mg cohort for the primary endpoint of placebo-adjusted mean change in 24-hour cough frequency at 12 weeks in COUGH-1 and 24 weeks in COUGH-2 were 18.5% (P = .041) and 14.6% (P = .031), respectively.
In a pooled analysis of COUGH-1 and COUGH-2, AEs reported in >5% of patients included dysgeusia (41.1%), ageusia (14.6%), hypogeusia (10.7%), nausea (9.4%), taste disorder (8.9%), cough (7.2%), dry mouth (6.6%), upper respiratory tract infection (6.3%), diarrhea (5.7%), and oropharyngeal pain (5.4%). Overall, 13.9% of patients discontinued therapy because of taste-related AEs.5,6
Based on clinical trial data, gefapixant was the first approved agent for RCC/UCC, available in the European Union, United Kingdom, Switzerland, and Japan. Therefore, HCPs in countries where gefapixant is approved may consider this agent after an informed discussion with patients about the risks and benefits of treatment. Taste-related AEs improve in 25% of patients and resolve in almost all patients after discontinuing therapy.1
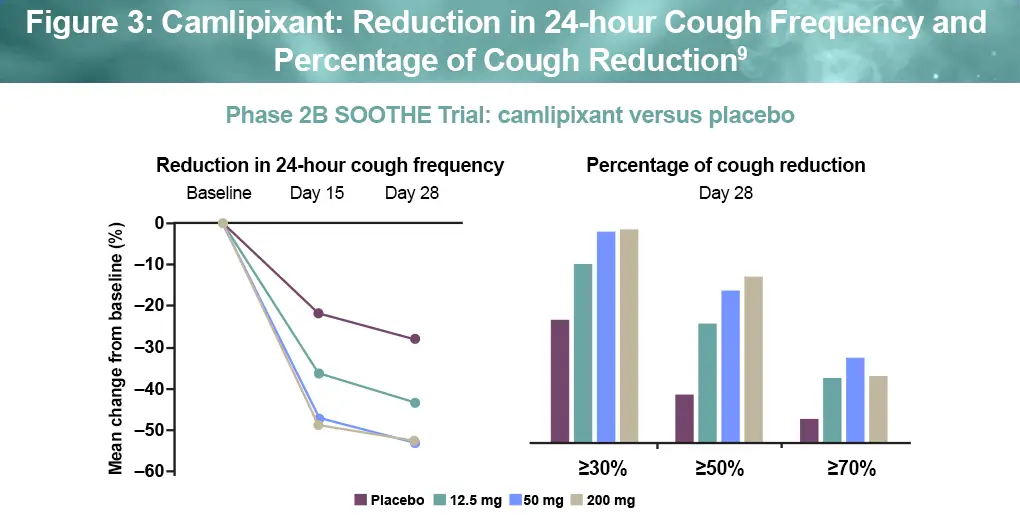
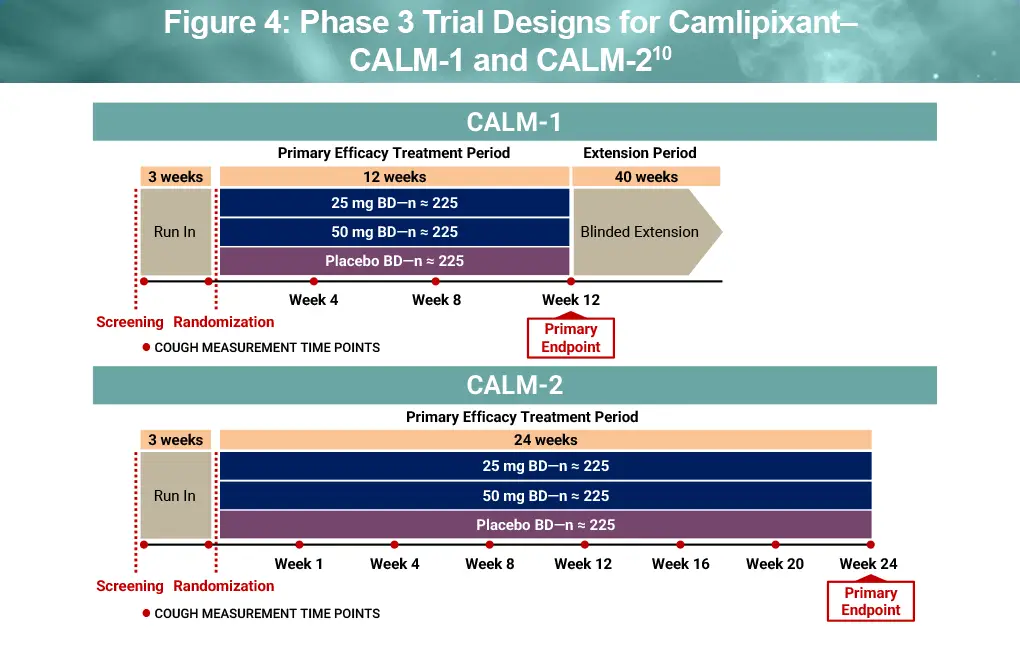
Camlipixant
Camlipixant, a second-generation P2X3 antagonist, has demonstrated efficacy and safety in a phase 2b clinical trial (see Figure 3).8,9 The phase 2B SOOTHE trial enrolled adults with RCC (cough duration ≥1 year; baseline awake cough frequency, ≥25 coughs/hour). Patients were randomized to one of three doses of camlipixant twice daily (12.5 mg, 50 mg, 200 mg) or placebo for 4 weeks (N = 310). Results showed a placebo-adjusted 24-hour cough frequency of 34% in both the 50-mg (P = .0033) and 200-mg arms (P = .0047). The incidence of treatment-emergent AEs was similar across all camlipixant and placebo arms. The most common treatment-emergent AEs were nausea and dysgeusia, with taste-related AEs reported in only 4.8% to 6.5% of patients.8,9
Other investigational agents
Nalbuphine, an oral κ-opioid receptor agonist/μ-antagonist, has demonstrated promising results in phase 2 trials, with phase 3 studies underway. Other investigational agents include sodium channel blockers, TRPM8 inhibitors, neurokinin 1 antagonists, and γ-aminobutyric acid β agonists, reflecting continued interest in mechanism-based therapies for RCC.7-9
References
- Satia I, Hassan W, McGarvey L, et al. The clinical approach to chronic cough. J Allergy Clin Immunol Pract. 2025;13:454-466.
- Gibson P, Wang G, McGarvey L, et al. Treatment of unexplained chronic cough: CHEST Guideline and Expert Panel Report. CHEST. 2016;149:27-44.
- Irwin RS, French CL, Chang AB, et al. Classification of cough as a symptom in adults and management algorithms: CHEST Guideline and Expert Panel Report. CHEST. 2018;153:196-209.
- Morice AH, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur Respir J. 2020;55:1901136.
- McGarvey LP, Birring SS, Morice AH, Dicpinigaitis PV, et al. Efficacy and safety of gefapixant, a P2X3receptor antagonist, in refractory chronic cough and unexplained chronic cough (COUGH-1 and COUGH-2): results from two double-blind, randomised, parallel-group, placebo-controlled, phase 3 trials. Lancet. 2022;399:909-923.
- Gefapixant. U.S. Food & Drug Administration Pulmonary-Allergy Drugs Advisory Committee. November 17, 2023. https://www.fda.gov/media/173927/download
- Irwin RS, Madison JM. Unexplained or refractory chronic cough in adults. N Engl J Med. 2025;392:1203-1214.
- Satia I. Management of refractory chronic cough and emerging therapies in 2025. Can Respirol Today. 2025;1:5-11. https://canadianrespirologytoday.com/article/view/1-2-Satia
- Smith JA, Birring SS, Blaiss MS, et al. Camlipixant in refractory chronic cough: a phase 2b, randomized, placebo-controlled trial (SOOTHE). Am J Respir Crit Care Med. 2025;211:1038-1048.
- Bellus Health Inc. Annual Information Form. Fiscal year ended December 31, 2022. https://www.sec.gov/Archives/edgar/data/1259942/000141057823000342/blu-20221231xex99d1.htm
All URLs accessed March 10, 2026
